Perinatal Hep B
- related: Hepatitis B
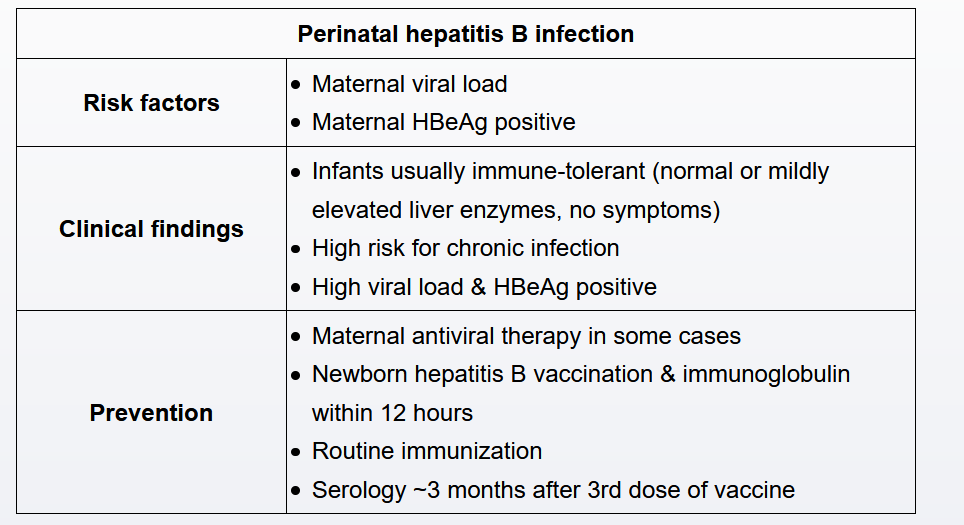
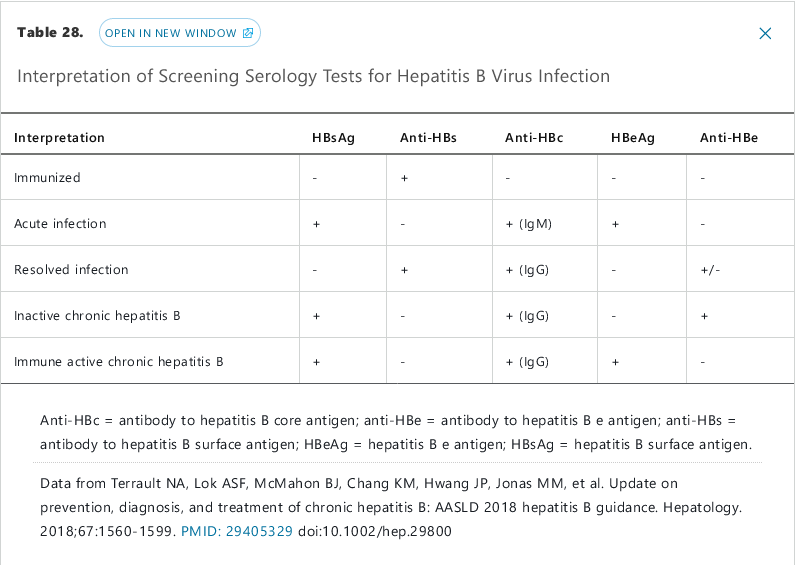
Infants born to mothers with active hepatitis B infection are at risk for acquiring hepatitis B either in utero or, more commonly, during delivery due to exposure to infected genital secretions. Maternal viral load is the primary risk factor and directly correlates with the risk of vertical transmission to the infant. However, with prompt administration of hepatitis B vaccine and immunoglobulin to the infant, the risk for infection decreases to <5%.
Infants who are vertically infected with hepatitis B generally develop chronic infection in an immune-tolerant phase. These infants characteristically have very high viral loads and positive HBeAg, but remain asymptomatic and have normal or minimally elevated liver enzymes. Therefore, liver function tests cannot be used to detect infection (Choice E). Instead, exposed infants should receive the hepatitis B vaccine and immunoglobulin within 12 hours of birth, followed by completion of the normal hepatitis B series (at age 0, 2, and 6 months). Serology should be obtained at the subsequent well-child visit, usually at age 9 months. If HBsAg is not detected at that time, the infant is uninfected.